Ligament Sprains and Tears - Prolotherapy is Effective
Ligaments connect bones to other bones. This tissue is meant to be strong in order to hold bones together and provide stability for the joint. While ligaments have a little “give”, they are not designed to be overly flexible. They can be overstretched, either suddenly, or gradually, resulting in a “sprain”. Sprains are common, and can be acute (sudden, short lived) or chronic (ongoing, recurrent). There are also degrees of sprain, all the way from mild to severe.
All three Prolotherapy formulas (Dextrose, PRP, Stem Cell) have shown a high success rate with ligament injuries and pain,[1] even when the sprain is old. This includes ankle sprains, [2] knee ACL (anterior cruciate ligament) MCL (medial collateral ligament) and meniscus tears[3] and other ligament sprains/tears.[4]
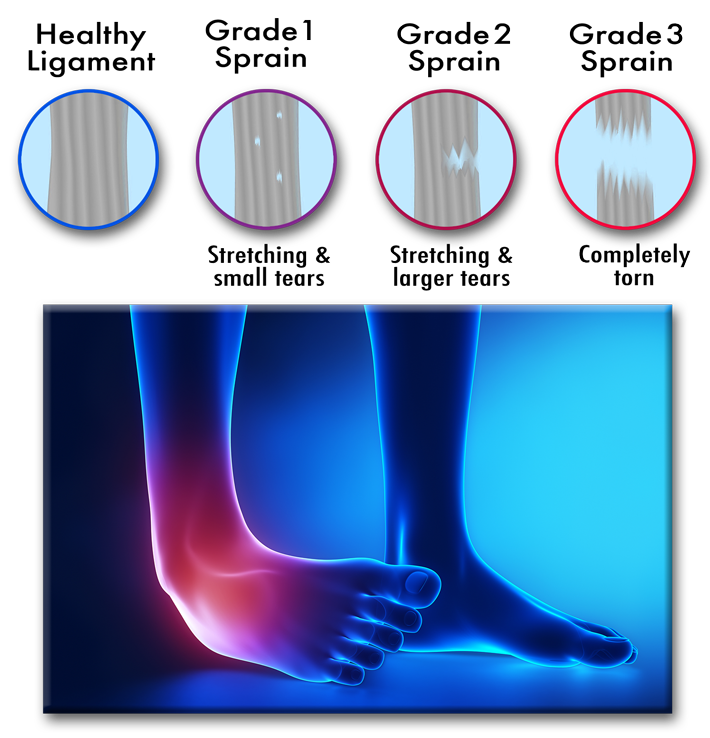
The system used by many doctors to determine the severity of a sprain ranges from Grade I (over-stretching) to partial tear (Grade II), then complete tear. If a ligament has a severe, complete tear (Grade III), surgery is often recommended, especially in cases where the injury is new and the demand on the joint is high, as in an active person or athlete. Fortunately, most sprains are Grade I or II and can be treated with Prolotherapy. And even in some cases of Grade III sprains, where surgery is not recommended, Prolotherapy has been successful.[5]
When it comes to complete ligament tears (Grade III), there is some controversy whether surgery should always be done, especially when injuries are older, or the individual is not very active. Although surgery for severe ligament injuries does appear to decrease the re-injury rate, it increases the risk for the subsequent development of osteoarthritis.[6] Balancing the advantages and disadvantages of surgical and nonsurgical treatment for ankle sprains specifically, authors in the Archives of Orthopedic and Trauma Surgery concluded that the majority of ankle sprains could be managed without surgery.[7]
Bibliography
[1] Hauser R, Hauser M, Cukla J. Dextrose prolotherapy injection for chronic ankle pain. Practical Pain Management. 2010; 10(1): 7–76; Van Pelt RS. Ankle and foot treatment with prolotherapy. Journal of Prolotherapy. 2011; 3(1): 576–581; Fullerton BD. High-resolution ultrasound and magnetic resonance imaging to document tissue repair after prolotherapy: A report of 3 cases. Archives of Physical Medicine and Rehabilitation. 2008 Feb 29; 89(2): 377–385
[2] Sinoff C. Prolotherapy for 20 year old ankle injury. Journal of Prolotherapy. 2010; 2(4): 497–488.
[3] Whyte GP, Gobbi A, Szwedowski D. Partial Anterior Cruciate Ligament Lesions: A Biological Approach to Repair. In Bio-Orthopaedics (pp. 665–670). Heidelberg, Germany: Springer. 2017; Chellis DM, Cortazzo MH. Regenerative medicine in the field of pain medicine: Prolotherapy, platelet-rich plasma therapy, and stem cell therapy—Theory and evidence. Techniques in Regional Anesthesia and Pain Management. 2011 Apr 30; 15(2): 74–80; Long term effects of dextrose prolotherapy for anterior cruciate ligament laxity. Alternative Therapies in Health and Medicine. 2003 May 1; 9(3): 58–62; Grote W, Delucia R, Waxman R, Zgierska A, Wilson J, Rabago D. Repair of a complete anterior cruciate tear using prolotherapy: a case report. International Musculoskeletal Medicine. 2009 Dec 1; 31(4): 159–165.
[4] Reeves KD, Hassanein KM. Fullerton BD, Reeves KD. Ultrasonography in regenerative injection (prolotherapy) using dextrose, platelet-rich plasma, and other injectants. Physical Medicine and Rehabilitation Clinics of North America. 2010 Aug 31; 21(3): 585–605; Hauser RA, Dolan EE, Phillips HJ, Newlin AC, Moore RE, Woldin BA. Ligament injury and healing: a review of current clinical diagnostics and therapeutics. Open Rehabilitation Journal. 2013 Jan 23; 6: 1–20; Ahmet Mustafa ADA MD, Yavuz F. Treatment of a medial collateral ligament sprain using prolotherapy: a case study. Alternative Therapies in Health and Medicine. 2015 Jul 1; 21(4): 68.
[5] Lazzara MA. The non-surgical repair of a complete Achilles tendon rupture by prolotherapy: biological reconstruction. A case report. Journal of Orthopaedic Medicine. 2005 Jan 1; 27(3): 128–132; Grote W, Delucia R, Waxman R, Zgierska A, Wilson J, Rabago D. Repair of a complete anterior cruciate tear using prolotherapy: a case report. International Musculoskeletal Medicine. 2009 Dec 1; 31(4): 159–165.
[6] Pihlajamäki H, Hietaniemi K, Paavola M, Visuri T, Mattila VM. Surgical versus functional treatment for acute ruptures of the lateral ligament complex of the ankle in young men: a randomized controlled trial. The Journal of Bone & Joint Surgery. 2010 Oct 20; 92(14): 2367–2374.
[7] Petersen W, Rembitzki IV, Koppenburg AG, Ellermann A, Liebau C, Brüggemann GP, Best R. Treatment of acute ankle ligament injuries: a systematic review. Archives of Orthopaedic and Trauma Surgery. 2013 Aug 1; 133(8): 1129–1141.